- Solve real problems with our hands-on interface
- Progress from basic puts and calls to advanced strategies
Interactive Options Course
Lesson 8 of 13
Contributed By: 
Summary
The following is a summary of a video recording and may contain errors in spelling or grammar. Although IBKR has edited for clarity no material changes have been made.
Hi, I’m Shea Wihlborg, the multiomics analyst here at ARK, and I’ll be walking through our Big Ideas for 2026 research for multiomics. I’ll start by defining what multiomics means and then walk through our research on the downstream implications for data generation, diagnostics, drug development, and therapeutics.

Multiomics reflects the fact that biology operates across multiple layers and that setting those layers together provides a more complete understanding of what shapes health, disease, and lifespan.
Rather than examining any single layer in isolation, multiomics is about capturing a systems-level view of biology. And while not limited to five, there are five core layers that are commonly referenced. Genomics refers to the DNA sequence. You can think of this as your underlying biological blueprint. Epigenomics captures modifications that regulate gene expression without actually changing the DNA sequence itself. Transcriptomics measures RNA transcripts, reflecting which genes are actively expressed in a cell.
Proteomics captures proteins, which carry out most of cellular functions. And metabolomics measures small molecules, such as sugars and fats, to reflect dynamic cellular activity. And together, these layers interact to shape phenotypes, the observable traits and outcomes of organisms like humans. There are companies working at different biological layers.
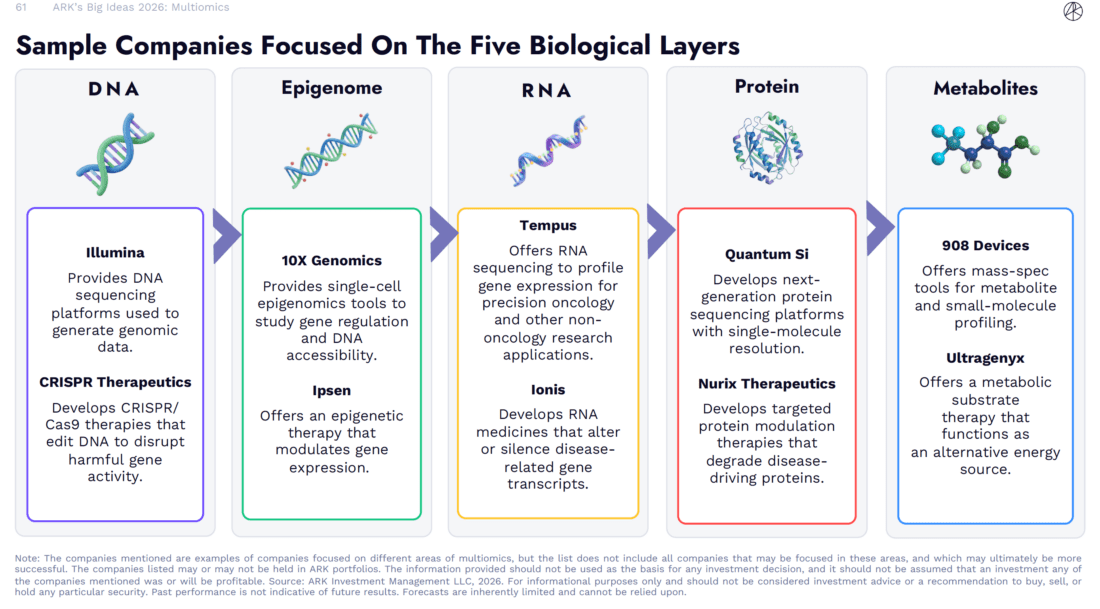
Some focused on a single layer, others spanning multiple layers to develop tools, diagnostics, and therapeutics. The takeaway is not the individual companies, but the breath of activity across the biological stack. Innovation is occurring simultaneously at multiple layers, which creates the conditions for integrating biological data and interventions across those layers.
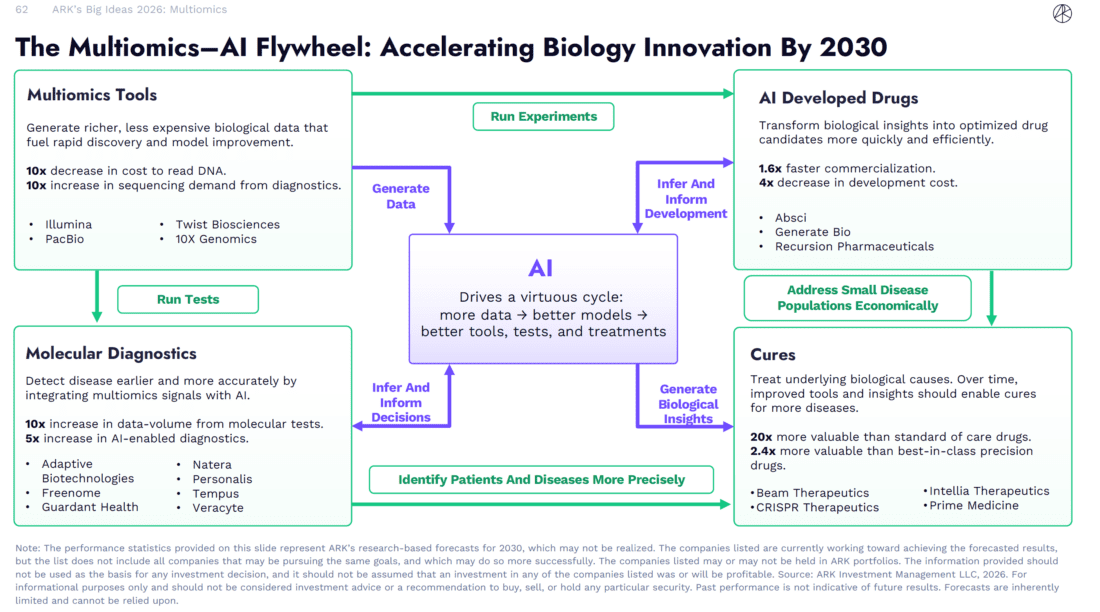
Artificial intelligence, or AI, introduces a reinforcing cycle in biology. As more biological data is generated, models improve. And as models improve, they enable better therapeutics, tools, and diagnostics, which in turn generate more and richer data. In effect,a virtuous cycle. We organize a cycle around four interconnected areas. First, multiomic tools, which are generating richer biological data at lower cost, expanding both the scale and resolution of measurement. Second is molecular diagnostics, which integrates multiomic signals to detect disease earlier and with greater precision. Third, AI-developed drugs, which use these biological insights to design and optimize drug candidates more efficiently. And finally, cures, represent the downstream consequence of improved biological understanding, treatments that target underlying disease mechanisms rather than just managing symptoms. And together, these areas reinforce one another as a multiomics AI flywheel. One of the most readily observable developments in multiomics is the rapid growth in biological data as costs decline. I’ll start by showing how this trend is playing out.
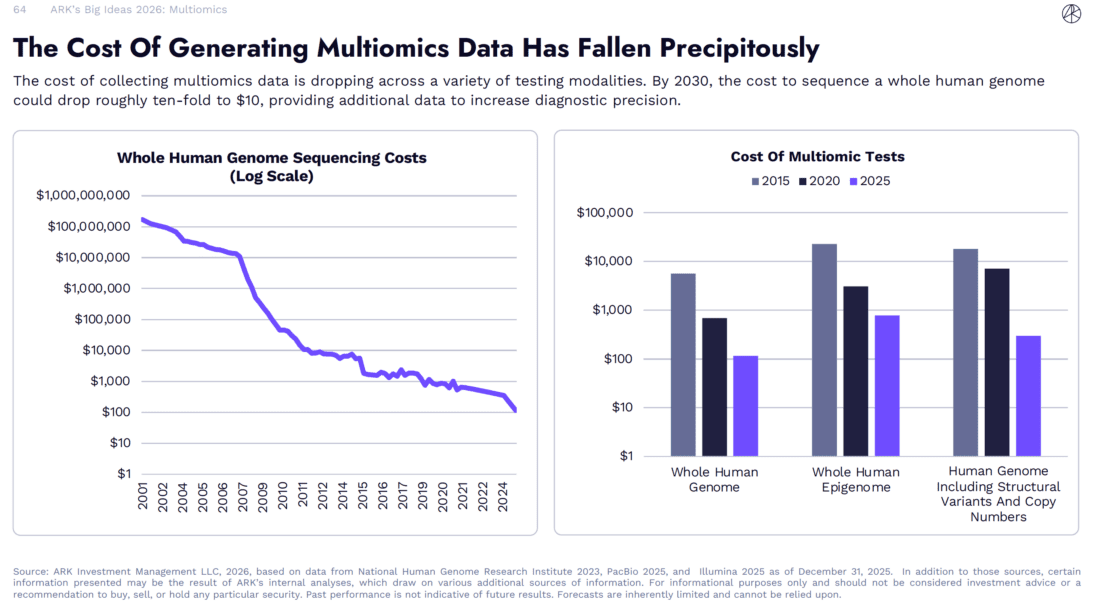
The first human-referenced genome sequence, i.e. the Human Genome Project, took about 13 years and cost approximately $2.7 billion to produce, including the infrastructure to do it all. Today, the cost to sequence a whole human genome has fallen dramatically and can be as low as around $100 per genome when done at scale. Based on continued declines in sequencing costs, our research suggests that by 2030, the cost could fall by another order of magnitude, reaching roughly $10 per genome. As test costs fall, test volumes increase.

Based on our modeling, the total number of next-gen molecular diagnostic tests should more than double by the end of the decade. As test volumes grow, so does the amount of biological data generated. To put that into context, on an annual basis, molecular diagnostics are generating token volumes that meet and then exceed the scale used to train frontier large language models from companies like OpenAI, Google, and Anthropic. Looking ahead, our modeling suggests this data volume will scale by tenfold by 2030.

On the note of AI, there is a clear inflection in AI-enabled diagnostics and medical devices beginning after late 2022. Since that point, the number of FDA approvals incorporating AI has increased meaningfully. Based on ARK’s best-fit modeling of approval trends, the share of AI-enabled diagnostics and devices is projected to rise from roughly 10 % today to about 30 % by 2030.
Next, let’s turn to how AI is changing the economics of drug discovery and development. Under the current industry standard, developing a new drug is a long, expensive, and highly uncertain process.

From initial discovery through regulatory approval, it typically takes more than decade, costs billions of dollars, and more than four out of every five drug candidates that enter clinical trials will ultimately fail. This combination of long timelines, high capital intensity, and low success rates has constrained productivity across the industry. In our research, AI represents a way to systematically address these constraints. Based on our modeling, AI-driven drug development has the potential to reduce time to market by roughly 40 % and total development costs by about fourfold. These gains can come from multiple points along the pipeline, from earlier stage design of higher quality drug candidates to improved biomarker development and more efficient patient matching during clinical trials.
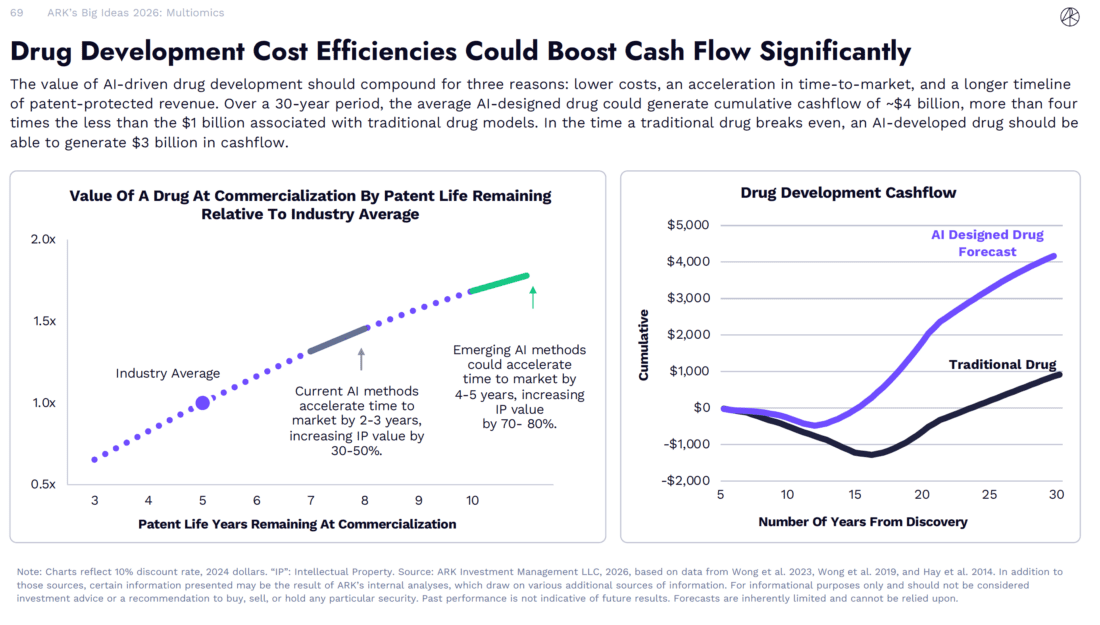
The value of AI-driven drug development ultimately comes down to two key factors. Lower development costs and faster time to market. And a faster time to market means a longer period of time of patent-protected revenue. By truncating both cost and time, our modeling suggests that an AI-developed drug could generate roughly 3 billion in cumulative cash flow before a traditional drug even reaches breakeven. And from ARK’s perspective, one of the most exciting and consequential developments in healthcare is the emergence of functional cures. A functional cure refers to a therapy that can durably eliminate disease activity after one time or a limited course of treatment rather than requiring lifelong management of symptoms. These therapies represent a meaningful departure from the traditional chronic care model with important clinical and economic implications. In ARK’s research, we model that because functional cures deliver most of their value upfront, they are priced significantly higher than traditional chronic therapies.

For rare diseases, our modeling suggests that the average price of a cure could exceed $1 million per patient, roughly 15 times the lifetime prescription costs required to manage the disease. By capturing revenue upfront, well before patent expiration, and by largely avoiding competitive overlap, cure’s front-load cash flows early in the commercial lifecycle. And ARK’s modeling this dynamic can make cures up to 20 times more valuable than a typical drug.
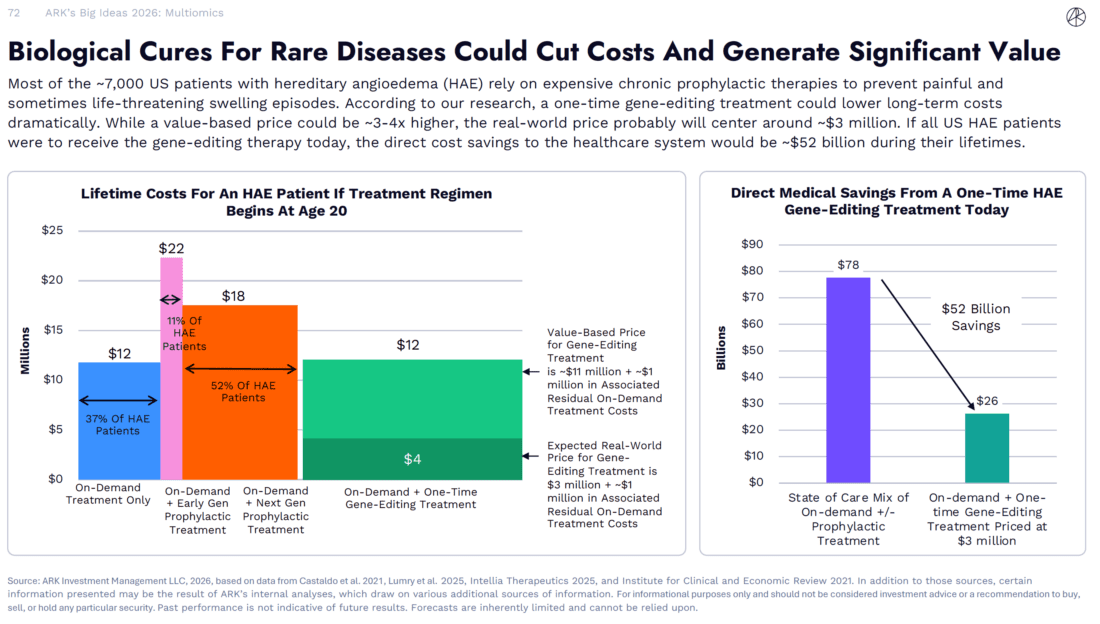
To make this concrete, ARK’s research looks at a case study in hereditary angioedema, or HAE, a rare genetic condition that can cause sudden, painful, and sometimes life-threatening swelling episodes. Today, most patients rely on a combination of chronic prophylactic treatments to reduce attack frequency and on-demand treatments to manage breakthrough episodes. Over a patient’s lifetime, the combined cost of having either on-demand or on-demand plus prophylactic treatment and the associated medical care that comes along with having HAE can reach roughly $10 to $20 million depending on the treatment regimen the patient takes.
In ARKs modeling, a one-time gene editing therapy currently in late-stage clinical development but not yet approved has the potential to more effectively prevent attacks with just a single administration. And gene editing therapies are beginning to move beyond rare diseases into common conditions, including cardiovascular disease, the leading cause of death globally.

A key enabler of this transition is the ability to perform gene editing in vivo or editing directly within the body. Emerging clinical data show that a one-time gene editing therapy can durably lower harmful lipid levels, lipids being the fat and fat-like molecules, which are a major driver of atherosclerotic cardiovascular disease. Using a Monte Carlo simulation, our research estimates a value-based price of approximately $165,000 for a one-time therapy that reduces lifetime cardiovascular risk. In the US, roughly 17 million patients have atherosclerotic cardiovascular disease, meaning they already have plaque buildup, and uncontrolled lipid levels despite available care. Applying that value-based price of $165,000 to this population of 17 million implies a total addressable market of about 2.8 trillion. For context, Pfizer statin Lipitor, used for cardiovascular disease was a blockbuster success and one of the best-selling drugs of all time for years. Capturing even one-twelfth of that TAM would match the cumulative sales of Lipitor over roughly 20 years. Given the high costs and low probabilities of success, returns on invested capital in traditional drug development are typically in the single digits.

Under this framework, early-stage assets, particularly at the phase one stage or earlier, tend to have limited to no economic value as most candidates fail before reaching commercialization. In ARK’s research, combining AI-driven reductions in development time with lower failure rates materially changes that profile. When those dynamics are applied to curative therapies, the expected value of assets earlier in development increases substantially. Based on ARK’s modeling, an AI-accelerated cure in its first phase of human testing could be worth more than $2 billion per drug.
Finally, I’ll turn to longevity. Longevity is sometimes associated with speculative therapies or cosmetic interventions, but the focus here is different. This section looks at longevity through the lens of biology, how advances in measuring and understanding the biology of aging are making it a more tractable scientific target.
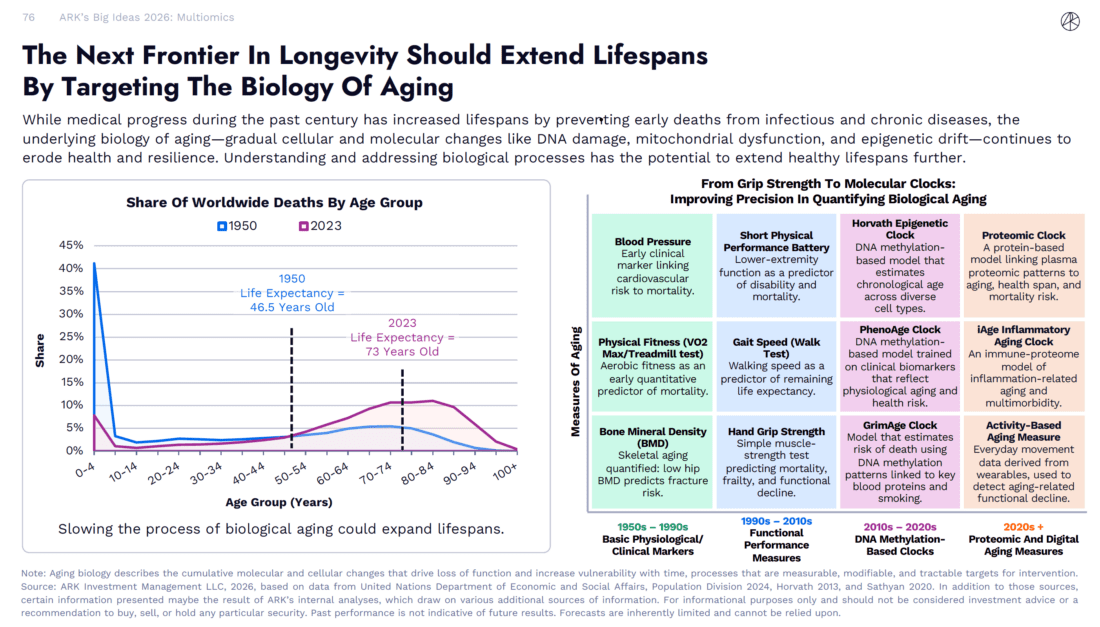
Over the past century, medical progress has meaningfully increased global lifespans, largely by preventing early deaths from infectious and chronic diseases. In 1950, global life expectancy was around 46 years. By 2023, it increased to roughly 73 years. Extending lifespans further increasingly depends on addressing the biological processes that elevate vulnerability with age. Aging is likely not driven by a single mechanism nor does it occur uniformly across individuals or even time. It reflects the gradual dysregulation of multiple cellular and molecular processes that reduce resilience, increase disease risk, and erode function over time. These processes occur across biological layers, such as DNA replication, gene regulation, protein function, and metabolism, across trillions of cells. While many repair mechanisms exist, errors still can accumulate over time influenced by both biology and environment. Importantly, our ability to measure biological aging has improved significantly. Earlier approaches relied on basic physiological and clinical markers such as blood pressure or bone mineral density. More recent measures in the 90s and early 2000s incorporated functional performance, including gait speed and grip strength.
Over the past decade or so, molecular clocks, first based on DNA methylation and more recently on proteomic and digital signals, have increased the precision with which aging can be quantified. As our understanding and measurement of the aging biology improve, aging becomes a more tractable target for scientific study, clinical evaluation, and medical intervention.
Information posted on IBKR Campus that is provided by third-parties does NOT constitute a recommendation that you should contract for the services of that third party. Third-party participants who contribute to IBKR Campus are independent of Interactive Brokers and Interactive Brokers does not make any representations or warranties concerning the services offered, their past or future performance, or the accuracy of the information provided by the third party. Past performance is no guarantee of future results.
This material is from ARK Invest and is being posted with its permission. The views expressed in this material are solely those of the author and/or ARK Invest and Interactive Brokers is not endorsing or recommending any investment or trading discussed in the material. This material is not and should not be construed as an offer to buy or sell any security. It should not be construed as research or investment advice or a recommendation to buy, sell or hold any security or commodity. This material does not and is not intended to take into account the particular financial conditions, investment objectives or requirements of individual customers. Before acting on this material, you should consider whether it is suitable for your particular circumstances and, as necessary, seek professional advice.









Join The Conversation
For specific platform feedback and suggestions, please submit it directly to our team using these instructions.
If you have an account-specific question or concern, please reach out to Client Services.
We encourage you to look through our FAQs before posting. Your question may already be covered!